ABSTRACT
Avascular necrosis (AVN) is a progressive disorder as a result of the death of cellular elements of bone due to the impairment or loss of blood supply to the bone. The condition also can be resulted due to the long term use of the high dose steroid medications, connective tissue disease,trauma,sickle cell disease etc. Commonly affecting sites includes the head of femur,humerus,proximal tibia and femoral condyles. Asthi-majjakshaya, usually presents with
symptoms asthitoda (bone pain) asthishathana (splitting of bone) and asthisoushiryam (osteoporosis) correlates with the symptoms of AVN. Administration of snehana (oleation therapy) both external and internal form is the best treatment modality in such case, especially vasthi with tiktarasa dravya processed in kshira is indicated. A 32 yr old lady patient presented with pain in her bilateral hip region since 2 years and also with difficulty in walking and doing
any activities was advised for surgery, approached our institution and the case was well managed and relieved markedly by pancharma procedures like Churna pinda sweda, Pathrapindasweda and by administering Panchatikta kṣīrabasti also by internal medicines .
INTRODUCTION
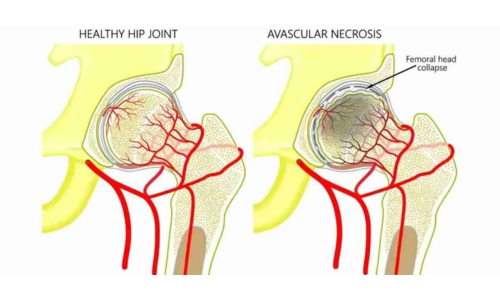
Avascular necrosis (AVN) is a disease resulting from a temporary or permanent loss of blood supply to the bones. It generally affects people between the ages of 30 and 50 years of age. This disease is also known as osteonecrosis, aseptic necrosis and ischemic bone necrosis. Avascular necrosis is the death of the bone marrow cells due to ischemia. In some cases, the bone will collapse. It affects the epiphysis of the long bones and is most commonly seen in the femur. Hip disease is bilateral in >50% cases. Clinical presentation is usually the abrupt onset of articular pain. Early changes are not visible on plain radiograph and are best seen by MRI,later stages demonstrate bone collapse (“ cresent sign”), flattening of articular surface with joint space loss.
CAUSES
Avascular necrosis has several causes. Trauma is the most common cause of AVN. It can occur within eight hours after a traumatic injury. The two most common etiologies of atraumatic avascular necrosis are alcohol consumption and long-term use of corticosteroids. Excessive alcohol consumption may have a toxic effect on osteogenic cells. The use of long-term steroids is associated with 35% of all cases of atraumatic avascular necrosis. Corticosteroid-related avascular necrosis is more severe and more likely to affect both hips than noncorticosteroid-related AVN.
AVN is also a side effect of other conditions, including Gaucher’s disease, pancreatitis, chemotherapy, hemodialysis, and blood disorders, such as sickle cell anemia.
According to ayurvedic concept unnatural vata prakopa leading to the depletion of the asthi dhathu as the asrayi-asraya bhava sidhantha2 which
results in the above said condition. According to Ayurveda, the causes like consumption of non- unctous substances, scanty intake of food, intake of foods which are light and cold by nature, indulging in more physical activities as well as mental strain like constant worrying and fear, default in the lifestyle and not following the healthy habits of daily routine dinacharya, vegasandharana (controlling the natural urges), rathrijagarana (sleeplessness) excessive travelling, traumatic conditions and injuries, excessive strenuous activities are the contributing causes for dhathukshaya3 and results in vata prakopa4. This vata prakopa further causes the manifestation of disease in the weakest dhathu or at the site of more kha vaighunyata in the shareera (body). Thus Kshaya in the asthimajja dhathus takes place due to the favourable nidana pertaining to the respective dhathu like lack of intake of asthi dhathu poshakamshas ( bone nourishing factors) like milk, ghee etc contributes to this disease. When we analyze the causative factors enlisted by
the contemporary science, it is highly evident that the basic concepts of the cause is more or less one and the same like dhathukshayajanya only.
SYMPTOMS
Avascular necrosis of the femoral head presents with groin pain that radiates down the anteromedial thigh. Some patients may demonstrate a limp and or limited range of motion in flexion, abduction and internal rotation. Pain is sometimes induced by standing, walking, moving or other mechanical stress. It’s usually relieved by rest. Symptoms of asthi-majjakshaya5 like asthi thoda (severe bone pain), asthisatana, asthisoushirya or hollowness in bone degenerative changes in the bone or osteoporosis) ,sandhishaithilya ( looseness in joints) are the main manifested symptoms of this disease.
DIAGNOSIS
A complete physical exam by a physician, including complete blood examination, family history, history of alcohol and/or long-term steroid use, as well as AP and lateral X-rays of the affected bone, is the first step in identifying AVN. This test would identify any abnormalities, such as inflammation, acute or chronic infection, and autoimmune disease. Total cholesterol examination may also be necessary to check on the amount of lipids in the blood. If the films show the presence of AVN, a series of additional imaging exams may be performed.
The tests listed here can be used to Progression of bonedetermine the amount of bone affected, as well growth.as the progression of the disease.
X-ray ,Magnetic resonance imaging (MRI), Bone scan, CT scan
AVN is classified by five stages through the use of normal radiological clinical findings. Each stage identifies and explains the pathological progress and the severity of the disease.
Stage 1: Cell death; undetectable by plain films
Stage 2: Cell modulation; characterized by localized osteoporois
Stage 3: Development of the margin of dead bone; appears sclerotic
Stage 4: Margin increases; takes on a crescent shape
Stage 5: Total destruction and possible collapse of the bone
CASE REPORT
A 32 year old female patient presented with pain in her bilateral hip region since 2 years and the pain was radiating to groin and further to the medial side of her thighs. The pain was pricking type and continuous in nature and aggravated during bending , walking and doing any activities and also during weight bearing. As time progresses she also experienced weakness of her lower limbs and the condition got worsened day by day. Modern medical science has advised her for surgery, but she refused and approached our institution for the better management without surgery.
Personal history:
- She had reduced appetite, mixed diet, constipated bowels and disturbed sleep.
Systemic examination
Musculoskeletal examination:
Hip joint :
Redness : Absent
Swelling : Absent
Temperature: Normal
Tenderness : Absent
Movements: all movements were restricted
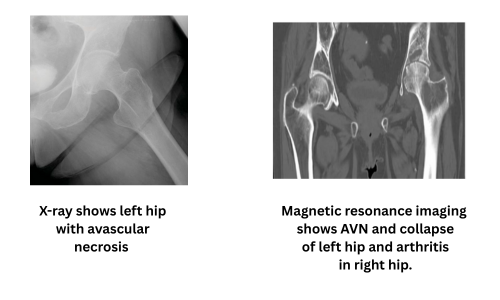
Investigations done: MRI :- pelvis including hip and sacroiliac joints revealed the following details:
Ø Subchondral sclerosis, cresent,collapse involving both femoral head
Ø Marrow edema involving both femoral head,neck and trochanteric regions
Ø Synovial effusion noticed in both hip joints.
Ø Possibility of modified FICAT ARLET stage 11b /111a avascular necrosis should be considered.
Treatment given:
Internal
- Amruthotharam kashaya6 90 ml bd
- Guggulutiktakam ghrita7
- Laksha guggulu8
- Gandha taila 910 drops with milk
External - Choorna pinda sweda with out oil for 3 days
- Choorna pinda sweda with dhanwantharam taila 10 and murivenna for 3 days
- Pathra pinda sweda for 14 days
- Panchatiktaksheeravasthi 11 for 5 days
RESULTS
| Sl. No | Subjective/Objective Parameter | BT | DAY 7 | DAY 14 | DAY 21 |
| 1 | Hip joint pain | 10 | 9 | 6 | 4 |
| 2 | Pain on raising from squatting | 10 | 9 | 6 | 5 |
| 3 | Pricking pain | 10 | 8 | 6 | 4 |
| 4 | Difficulty in walking | 9 | 8 | 6 | 3 |
| 5 | Stiffness | 9 | 7 | 4 | 3 |
The assessment was done before and after the completion of treatment. Patient got 60% relief in 4 parameters and 50% relief in one parameter within a span of 21 days of treatment. The bilateral hip joint pain which was pricking in nature was found to be reduced remarkedly and in the VAS score has come to 4 from 10.difficulty in walking and stiffness of the joint also reduced by 60%.pain on raising from squatting has reduced by 50%.
DISCUSSION
Avascular necrosis of femur head is the condition which is primarily due to the lack or loss of blood supply and this can be understood through Ayurvedic perspective as asthi-majja dhathukshaya due to the deprivation of nutrients to the asthi dhathu and thereby leading to the uthara dhathu depletion ie.majjakshaya also. The treatment strategies for aggravated vata includes oleation therapies both internally and externally,sudation therapy and timely mild purificatory therapies . Among all therapies, vasthi is the excellent therapy for mitigating vata as it can conquer the prakupita vata immediately by reaching the visesha sthana of vata quickly and directly. ie.pakwashaya. The treatment protocol for asthimajja kshaya is the administration of various panchakarma procedures and especially vasthi using milk and ghee of tikta rasa (bitter taste) . Hence in this case we administered panchatiktaksheera vasthi so as to promote the asthi
dhathu. Daily intake of milk and ghee also plays a key role in the regeneration of the asthimajja dhathus effectively.
Guggulu tiktaka gritha which is highly persuasive in mitigating the asthimajja vikaras was given as mathra vasthi helps in the restitution of the asthi and majja dhathus. Since the patient was having reduced appetite and constipation Amruthothara kashaya was given for the amapachana and for anulomathva of the vata. Guggulu tiktaka gritha is specially indicated in asthisandhimajja vikaras which comprises of thikta dravyas, hence given as a samana sneha. Laksha guggulu was given to the patient as the preparation is excellent in asthi sandhanakara( bone remodeling ) and
also prevents the bone from getting pathological fracture. Gandha taila which is the best yoga for asthisthairyakara (one strenghthening ) serves the purpose of asthiposhana thereby minimize the pain and weakness in the asthi.
Ayurvedic concept emphasize that it is most important to have timely food that have a balancing effect on the `dominant dosha, and thereby pacify (stabilize) a dosha that has become excessive or aggravated. Since Vata is having rooksha sheetha laghu guna (qualities like drying, cooling and light) it is preferable to take foods which are snigdha,ushna,and guru gunas (unctuous,warm and heavy quality). The excellent tastes to pacify Vata includes sweet, salty, and sour. Hence foods having these taste has to be advocated to the mitigation of vata in the form of meat soups, porridges with milk, meat added with fats (ghee or oil) should be included in the diet . Intake of foods that are pungent, bitter, or astringent should be minimized or avoided. Suppression of natural urges and constant mental strain which immediately increases vata should be avoided.
CONCLUSION
The case report revealed that the AVN condition can be managed and recouped betterly through the ayurvedic treatment modalities like panchakarmas as well as with internal supplementation of guggulutiktaka ghrita,laksha guggulu and gandha taila. It serves as an effective remedy with an improvement in the quality of the patients life by minimizing the disabilities to a greater extend. However , more number of cases has to be studied to generalise the effect of the treatment protocol. Researches are still under trial in such cases. A wholistic approach to the patient with
further modifications in the diet pattern which is promoting the asthi majja dhathus, daily intake of milk and ghee, with the healthy life styles, administering adequate medicines and panchakarma therapy can further yield a better result in such similar cases.
REFERENCES
- Longo, Fauci, Kasper et. al., Hand book of Harrisson’s Principles of Internal Medicine, 18th Edition, ,Pp: 1550Pg: 1098
- Vagbhata, Astanga Hrudaya, Sarvanga Sundara Commentary of Arunadatta and Ayurveda Rasayana Commentary of Hemadri, edited by; Pandit Hari Sadasiva Sastri Paradikara Bhisagacharya, Choukambha Surabharati Prakashan, Varanasi, reprint-2010, Pp: 956, Pg.186
- Agnivesha, Charaka Samhita, Ayurveda Deepika Commentary of Chakrapani, edited by; Vaidya Yadavji Trikramji Acharya, Choukambha Surabharati Prakashan, Varanasi, reprint-2011, Pp: 738, Pg.619
- Agnivesha, Charaka Samhita, Ayurveda Deepika Commentary of Chakrapani, edited by; Vaidya Yadavji Trikramji Acharya, Choukambha Surabharati Prakashan, Varanasi, reprint-2011, Pp: 738, Pg. 617
- Agnivesha, Charaka Samhita, Ayurveda Deepika Commentary of Chakrapani, edited by; Vaidya Yadavji Trikramji Acharya, Choukambha Surabharati Prakashan, Varanasi, reprint-2011, Pp: 738, Pg.103
- Sahasrayogam, jwara prakarana.
- Vagbhata, Astanga Hrudaya, Sarvanga Sundara Commentary of Arunadatta and Ayurveda Rasayana Commentary of Hemadri, edited by; Pandit Hari Sadasiva Sastri Paradikara Bhisagacharya, Choukambha Surabharati Prakashan, Varanasi, reprint-2010, Pp: 956, Pg.726
- Shri Govinda Dasji,Bhaishajya Ratnavali,commentary by Shri Kaviraja Ambikadatta Shastri,edited by Bhisagratna ShriBrahmashankar Mishra ,Vol 2 , Choukambha Surabharati Prakashan, Varanasi, reprint-2014, Pp: 799, Pg.774
- Vagbhata, Astanga Hrudaya, Sarvanga Sundara Commentary of Arunadatta and Ayurveda Rasayana Commentary of Hemadri, edited by; Pandit Hari Sadasiva Sastri Paradikara Bhisagacharya, Choukambha Surabharati Prakashan, Varanasi, reprint-2010, Pp: 956, Pg.876
- Vagbhata, Astanga Hrudaya, Sarvanga Sundara Commentary of Arunadatta and Ayurveda Rasayana Commentary of Hemadri, edited by; Pandit Hari Sadasiva Sastri Paradikara Bhisagacharya, Choukambha Surabharati Prakashan, Varanasi, reprint-2010, Pp: 956, Pg.383
- Vagbhata, Astanga Hrudaya, Sarvanga Sundara Commentary of Arunadatta and Ayurveda Rasayana Commentary of Hemadri, edited by; Pandit Hari Sadasiva Sastri Paradikara Bhisagacharya, Choukambha Surabharati Prakashan, Varanasi, reprint-2010, Pp: 956, Pg.726
Case study done by Dr. Parvathy Ravindran, AYURDEVA – Multi Specialty Ayurvedic Centre, Kochi: Phone:+91 94006 39699


